


Analysis: The potential disadvantages of drugs increasingly used by patients to achieve greater weight loss are often not highlighted
Obesity is becoming increasingly common worldwide. Glucagon-like peptide-1 Receptor Agonist (GLP-1RA) type drugs like Ozempic (semaglutide) and Mounjaro (tirzepatide) can help patients achieve greater weight loss than most other drugs which are licenced for this purpose. Several benefits have been described in the short term, especially relating to diseases associated with obesity.
But the drugs are frequently promoted uncritically on social media and even in the medical press. Unfortunately, much of the published evidence on the drugs is also sponsored by the pharmaceutical companies who manufacture and sell them. Hence, the potential adverse effects of the drugs are often not highlighted.
We need your consent to load this rte-player contentWe use rte-player to manage extra content that can set cookies on your device and collect data about your activity. Please review their details and accept them to load the content.Manage Preferences
From RTÉ Radio 1's Liveline, listeners call in to discuss their experiences with drugs like Ozempic
What is needed is a balanced, evidence-based account of the potential downsides of these drugs. This is essential to empower anyone thinking of commencing them to arrive at an informed decision.
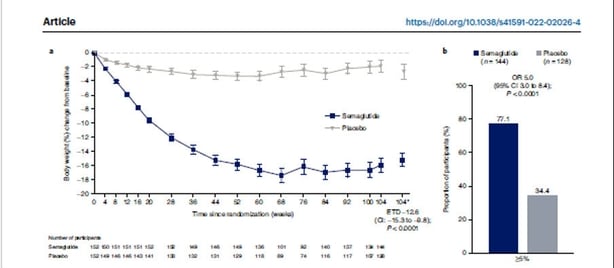
Levelling out of weight loss within one year of treatment
Weight loss on these drugs plateaus after approximately 12 months. This is shown very clearly in a recent research paper looking at the effects of giving one such drug (Semaglutide) over a 2 year period. The grey line is the placebo group who did not receive any active drug, while the navy line tracks the weight of the group receiving the GLP-1RA drug. It is clear that weight loss plateaued halfway through the study and no further loss was achieved.
Adverse effects
Well described adverse effects include nausea and vomiting which has been reported in over 80% of patients taking Semaglutide and 6% of those taking Tirzepatide. This can lead to dehydration and malnutrition. Reduced efficacy of oral contraceptives can occur. Rarer adverse effects include inflammation of the pancreas and thyroid gland tumours.
The discontinuation rate
A certain proportion of patients who start the drug do not continue with it. This is known as the discontinuation rate. The numbers vary and are lower in trials sponsored by the drug's manufacturers. However, independent studies show rates of discontinuation of up to 60% by the end of one year. Because of early discontinuation of the drug, the effective weight loss is often less than that shown in industry sponsored trials. For example, several studies have shown that 15% of weight loss only occurs in between 20% and 40% of those started on the drug.
Lean mass loss
Lean Mass is made up of muscle and bone. As we age, there is a gradual falloff in muscle which starts at age 30 and accelerates after age 60. Low muscle strength is associated with a higher risk of dying. While all methods of weight loss will involve some degree of lean mass loss, the potency of these drugs mean that the amounts lost are much higher. The figures vary from 14% to 39% of weight loss. This level of lean mass loss has been equated to a decade of human ageing. Although there is no evidence to show harm, loss of lean mass can lead to increased falls and fracture risk.
We need your consent to load this rte-player contentWe use rte-player to manage extra content that can set cookies on your device and collect data about your activity. Please review their details and accept them to load the content.Manage Preferences
From RTÉ Radio 1's Drivetime, concerns over illegal or fake versions of Ozempic
It is recommended that those who decide to go ahead with GLP-1RA-like medication should participate in comprehensive treatment programs emphasizing adequate protein and micronutrient intakes, as well as resistance training, to preserve muscle mass and function. Close monitoring of mobility, physical activity, and activities of daily living is essential, especially in patients aged 65 years or older.
Weight regain after treatment ends
Cessation of therapy is often followed by weight regain. In one trial, participants had regained two-thirds of their prior weight loss one year after withdrawal of once-weekly subcutaneous semaglutide 2.4 mg and lifestyle intervention. Other studies have also shown a rapid regain of weight after cessation of therapy, regardless of the duration of the treatment. There is a risk of much of this regain being fatty tissue with little regain of lean mass. The body’s capacity to rebuild lean tissue can be impaired by aging and malnutrition.
Weight cycling
Weight cycling occurs where people repeatedly start and stop taking these drugs. Having lost weight on the drug, they regain weight on cessation. They then restart the drug and lose further weight, but then stop the drug again and the cycle repeats. There is a risk here that both fat and lean mass are lost during the weight loss cycle, but the weight regained may be mostly fat. In a recent review on this topic, five of 20 studies included showed an association between weight cycling and increased fat mass while 15 did not.
We need your consent to load this rte-player contentWe use rte-player to manage extra content that can set cookies on your device and collect data about your activity. Please review their details and accept them to load the content.Manage Preferences
From RTÉ Radio 1's Drivetime, Ozempic shortage pitting diabetic patients against people with obesity
The risk is that certain vulnerable patients may gain fat mass at the expense of lean mass as time goes on, resulting in reduced muscle mass (known as sarcopenia) and thinner bones. This can lead to a medical condition called "sarcopenic obesity" which is unhealthy.
Malnutrition
Thiamine deficiency, acid base imbalance, starvation, food craving and low blood sugar levels have been described with the drugs. It is important to counsel patients contemplating GLP-1 RA treatment on the risks of malnutrition after unsupported dietary restriction. Dietary recommendations to support effective GLP-1 RA type drug therapy have been made. Monitoring for micronutrient deficiency is also recommended. An excellent, freely available and easily understandable paper gives a short and comprehensive summary on what everyone should know before starting a course of GLP-1 RA drugs.
GLP1-RAs should only be initiated with along with a supervised exercise programme and individualised dietetic advice. Subsequent patient monitoring to detect cessation, malnutrition and inappropriate fatty tissue weight gain is recommended.
Follow RTÉ Brainstorm on WhatsApp and Instagram for more stories and updates
The views expressed here are those of the author and do not represent or reflect the views of RTÉ. If you have been affected by issues raised in this article, support information is available online
