










































In an editorial that might have been written in 2020, the Freeman's Journal of 20 May 1847 acknowledged the 'semblance of action' that was being taken by the authorities at the height of a 'famine fever' epidemic in Dublin, but criticised the absence of any measures to halt the spread of the disease.
Temporary fever hospitals were being erected and medical officers appointed to administer 'all the appliances of cure', but those patients turned away by the overcrowded hospitals, 'returned to their gloomy, ill-ventilated, over-crowded abodes' to disseminate contagion in their districts. 'Is it not time', he demanded, 'to organise a Sanatory Police!'
While malnutrition certainly provided a weakened host, most famine-related diseases thrived due to the unsanitary and cramped living conditions of the poor. Typhus and relapsing fever, the most prevalent forms of what was commonly known as 'famine fever,' were carried by lice and spread through close contact.

Morphological characteristics of the body louse (Pediculus humanus corporis), carriers of the epidemic typhus, trench fever, and relapsing fever, 1972. Image courtesy Centers for Disease Control (CDC). Source:Collection/Gado/Getty Images
As the destitute poor took to the roads in search of relief, the lice found new hosts at soup kitchens, public works and in the country's prisons and workhouses. The exhausted victims of fever were also susceptible to other epidemic diseases such as dysentery, smallpox and tuberculosis.
Ireland's medical institutions were entirely unequipped to deal with the scale of the emergency. County and district fever hospitals were overcrowded, underfunded and unevenly distributed across the country.
Medical charities, which provided a network of dispensaries and fever hospitals, were entirely dependent on dwindling philanthropy and unable to meet the demands of a national epidemic. In line with the general policy of limiting state intervention, the government refused to provide emergency funding for existing fever hospitals and dispensaries.
It concentrated instead on increasing the role of the Poor Law Commission in the provision of medical care. In just six years between 1845 and 1851 many permanent institutions were driven to bankruptcy and closure while the number of fever hospitals and dispensaries attached to poor law union workhouses increased exponentially.
Increasing alarm
By the spring of 1846 reports from medical officers in the poorest areas of the country were becoming increasingly urgent in tone. Their resources were already stretched, and they doubted their ability to deal with the predicted health crisis.
![Sir James Graham (1792-1861) circa 1840s. From "Cassell's History of England - Special Edition, Vol. V [Cassell and Company, Limited, London, Paris, New York & Melbourne, circa 1890]. Source: The Print Collector/Heritage Images via Getty Images](https://www.rte.ie/images/001624da-1600.jpg)
Sir James Graham (1792-1861) circa 1840s. From "Cassell's History of England - Special Edition, Vol. V [Cassell and Company, Limited, London, Paris, New York & Melbourne, circa 1890]. Source: The Print Collector/Heritage Images via Getty Images
On 13 March, Tory Home Secretary Sir James Graham introduced a bill to 'make temporary provision for the treatment of destitute persons affected with fever in Ireland'. Enacted on 24 March, it provided for a temporary Central Board of Health to coordinate the medical response and to hire medical officers to serve in the regions most affected by disease.
The board comprised Sir Randolph Routh, an army commissary officer and chairman of the Central Relief Commission; Chief Poor Law Commissioner Edward Twistleton, and three prominent Dublin physicians, Sir Robert Kane, Sir Philp Crampton and Dominic Corrigan.
This body had the power to compel boards of guardians to establish fever hospitals and dispensaries and to provide food, medicine and bedding for the patients. The Treasury loans, advanced to cover the establishment and maintenance of temporary fever hospitals, were to be repaid from local poor rates.
Judiciously conceived?
The Londonderry Journal of 25 March hailed the temporary fever act as very important and 'very judiciously conceived'. In practice however, it had many deficiencies. Its greatest failing was that it placed the whole expense on rate payers and relied too heavily on local initiative. In spite of growing distress, only seventeen requests for intervention had been received by 1 September 1847 when the act expired.
The board, which disbanded in August, concluded that the summer had 'passed over without producing much alarm', but warned Sir John Russell's new Liberal government that the incidents of disease were likely to increase during the winter. Russell decided not to renew the legislation and when fever hit hard the following winter the government was unprepared to deal with it.
Sir John Russell. Source: Universal History Archive/Universal Images Group via Getty Images
National epidemic
After the more virulent and widespread blight of 1846, localised food shortages had given gave way to widespread distress and, by winter, the sporadic outbreaks of fever had become a national epidemic. Typhus and relapsing fever swept through the population and British and Irish newspapers published eyewitness accounts of the alarming progress of famine-related diseases. According to the report of the Poor Law Commissioners in December 1846:
In Connacht and the south of Ireland such has been the frightful state of distress that the workhouses were crowded to an extent far beyond their calculated capacity and disease has been introduced by persons suffering under dysentery and fever, and has spread to the inmates and officers who were previously healthy …
In the present state of things nearly every person admitted is a patient; separation of the sick by reasons of their number becomes impossible; disease spreads and by rapid transmission the workhouse is changed into one large hospital.
Ireland's cities came under increasing pressure from October 1846. Overcrowded workhouses and hospitals teemed with fever-stricken inmates as even more famine migrants arrived seeking succour. 'One-third of the daily population' on Cork city's streets, wrote Dr Callaghan in August 1849, 'consisted of shadows and spectres, the impersonations of disease and famine.'
In January 1847, William E. Forster of the Society of Friends (Quakers) despaired that the people of Louisburgh in County Mayo were 'being swept off by dysentery' in numbers as large as 'ten to twenty a day'. On the 5 March, the Freeman's Journal's west Cork correspondent claimed that
'there is not a house from Bantry to Schull that, with scarce a dozen exceptions, does not contain either the sick, dying or the dead … None of the peasantry, for the world's wealth, would go near the bodies, such is their apprehension of contagious fever.'
The journalist appealed to the authorities to provide doctors and hospitals if they wanted to prevent 'the whole south west of Cork from becoming a universal graveyard'.
The Famine memorial at Abbeystrowry Cemetery in Skibbereen, West Cork. Photo by: Education Images/Universal Images Group via Getty Images
A new emergency
In the face of the new emergency, the Central Board of Health was reappointed in February 1847. A second temporary fever act was passed in April transferring responsibility for local emergency fever hospitals and dispensaries from the poor law guardians to local relief committees.
Funded by local subscriptions, matched by government grants, these committees also assumed the cost of establishing and maintaining hospitals and paying the salaries of the medical officers. Although it was an improvement on the earlier legislation, this arrangement did less than was needed to augment the levels of medical relief for the poor in Ireland.
Nonetheless, it remained in place until 1850 when the Central Board of Health disbanded and the temporary fever act expired.
As well as a stream of correspondence highlighting the inadequacy or absence of medical facilities, the board received hundreds of applications for intervention from local committees. Medical inspectors such as Dr Richard Stephens were dispatched to the provinces to inspect and report on the state of the workhouses and by 17 August, 326 temporary fever hospitals and dispensaries had been authorised.
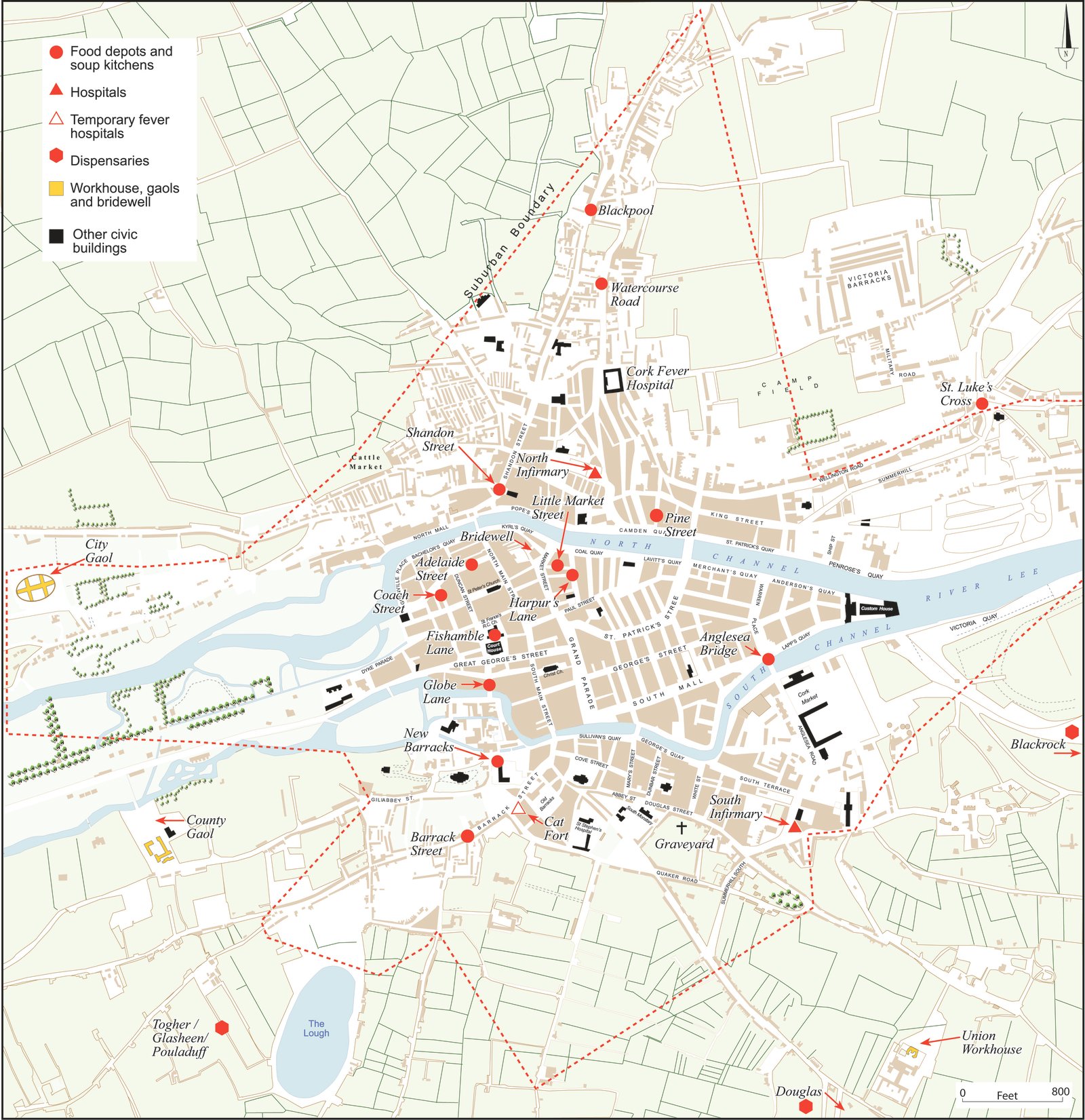
Location of medical and relief facilities and burial grounds in Cork City during the Famine. Map taken from the Atlas of the Great Irish Famine edited by John Crowley, William J. Smyth and Mike Murphy
The Board recommended that existing buildings should be converted for use as emergency fever hospitals or, where that was not possible, wooden fever sheds constructed, based on the economical designs by the Poor Law Commission's architect, George Wilkinson.
Between July 1847, when the board began to receive weekly returns, and August 1850, when it was disbanded, 579,721 patients were treated in temporary fever hospitals with an average mortality of 10.4 percent. This is not a representative figure, however, as the vast majority of fever victims, fearful and suspicious of the public health facilities, never entered the hospitals.
The Board of Health refused to sanction visits by medical officers to the patients' homes on the grounds that they were 'often scattered over an extensive district' and attending to the victims of fever 'lying with the families in ill-ventilated cabins' would increase the transmission of the disease.
Frontline workers
Clergy and voluntary relief workers, who did visit the homes of the sick, made enormous efforts to ameliorate suffering. Unlike the ravages of famine, however, typhus did not distinguish between classes and these front line workers, as well as the medical and administrative staff in workhouses and fever hospitals, often fell victim to the contagious disease.

An engraving depicting Father Mathew (Theobald Mathew 1790-1856) comforting a starving family during the Famine. Source: Universal History Archive/Universal Images Group via Getty Images
On 22 May 1847, for example, the Kerry Evening Post printed the obituaries of 'two excellent gentlemen'. Dr Henry Soden died of typhus 'caught while discharging his professional duties in [Mohill] workhouse' and Reverend James Flynn, curate of an adjoining parish, 'contracted typhus while administering the last rights to the dying poor'.
The famine fever epidemics had waned by mid-1848, but mortality rates spiked again after an outbreak of cholera in November. Fever returned sporadically in 1849 and 1850 and persisted in places even after the temporary legislation was allowed to lapse in August.
Approximately one million people died during the Famine. Some died of starvation, others of nutritional deficiencies, but the great majority were swept away by infectious disease.
This piece is part of the Great Irish Famine project coordinated by UCC and based on the Atlas of the Great Irish Famine. Its contents do not represent or reflect the views of RTÉ.





